What are Eosinophilic Gastrointestinal Diseases (EGIDs)?
Eosinophilic gastrointestinal diseases (EGIDs) occur when a type of white blood cell, called an eosinophil (pronounced ee-oh-sin-oh-fill), is found in increased numbers in the gastrointestinal tract.
Eosinophils are an important cell in your body. It has many roles including defence against parasitic infections (e.g. worms), and involvement in some forms of hypersensitivity and allergy. In some individuals, eosinophils accumulate in the gut, potentially in response to drugs, food, airborne allergens and other unknown triggers. This infiltration can cause inflammation and tissue damage.
In EGIDs, if an increased number of eosinophils are found in different regions it is called:
In EGIDs, if an increased number of eosinophils are found in different regions it is called:
- eosinophilic oesophagitis (EoE) - oesophagus
- eosinophilic gastritis (EoG) - stomach
- eosinophilic duodenitis (EoD) - duodenum
- eosinophilic enteritis (EoN) - small bowel/intestine
- eosinophilic colitis (EoC) - colon/large intestine
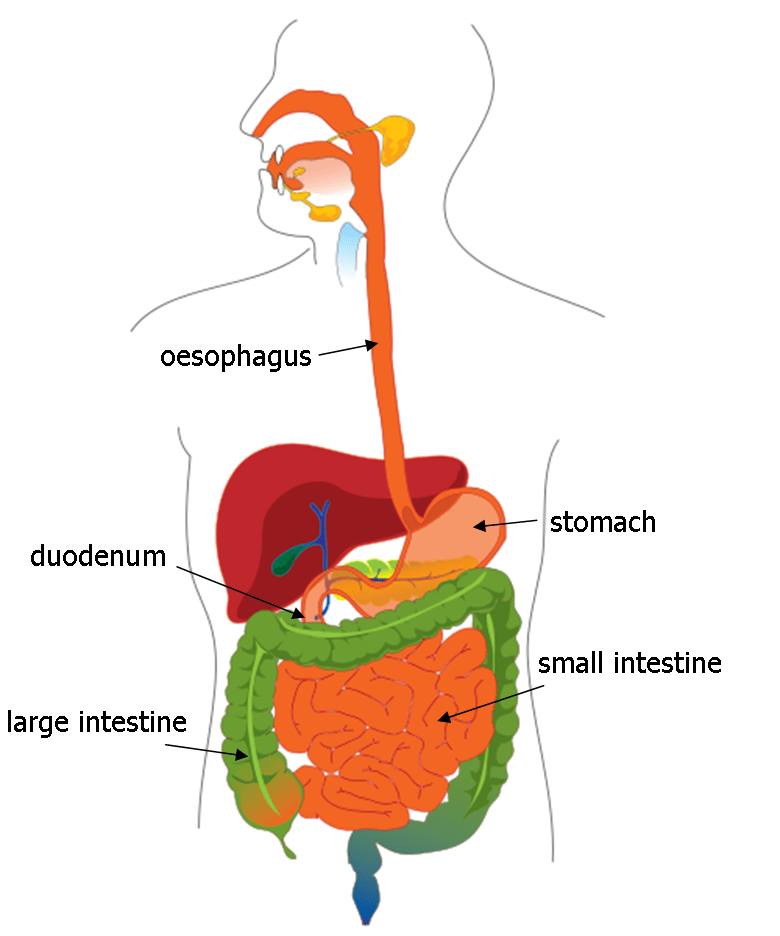
gastrointestinal (GI) tract
What is Eosinophilic Oesophagitis (EoE)?
Eosinophilic Oesophagitis (EoE) is the most known type of EGID, where the eosinophilic infiltration is in the oesophagus (food pipe that connects the mouth to the stomach).
The exact cause of EoE in most individuals is unclear. In some, it appears to be due to an allergy to food(s) and/or aero-allergens.
The current estimated prevalence of EoE is 1 in 1,000 individuals and rising. People with EoE may have other allergic diseases such as IgE (immediate) food allergies, asthma, eczema and/or hay fever. EoE affects people of all ages, sex and ethnicity. In some families, there may be an inherited (genetic) tendency. Males are more commonly affected than females.
In its most severe form, EoE may cause fibrous scar tissue in the oesophagus resulting in strictures (narrowing).
The current estimated prevalence of EoE is 1 in 1,000 individuals and rising. People with EoE may have other allergic diseases such as IgE (immediate) food allergies, asthma, eczema and/or hay fever. EoE affects people of all ages, sex and ethnicity. In some families, there may be an inherited (genetic) tendency. Males are more commonly affected than females.
In its most severe form, EoE may cause fibrous scar tissue in the oesophagus resulting in strictures (narrowing).
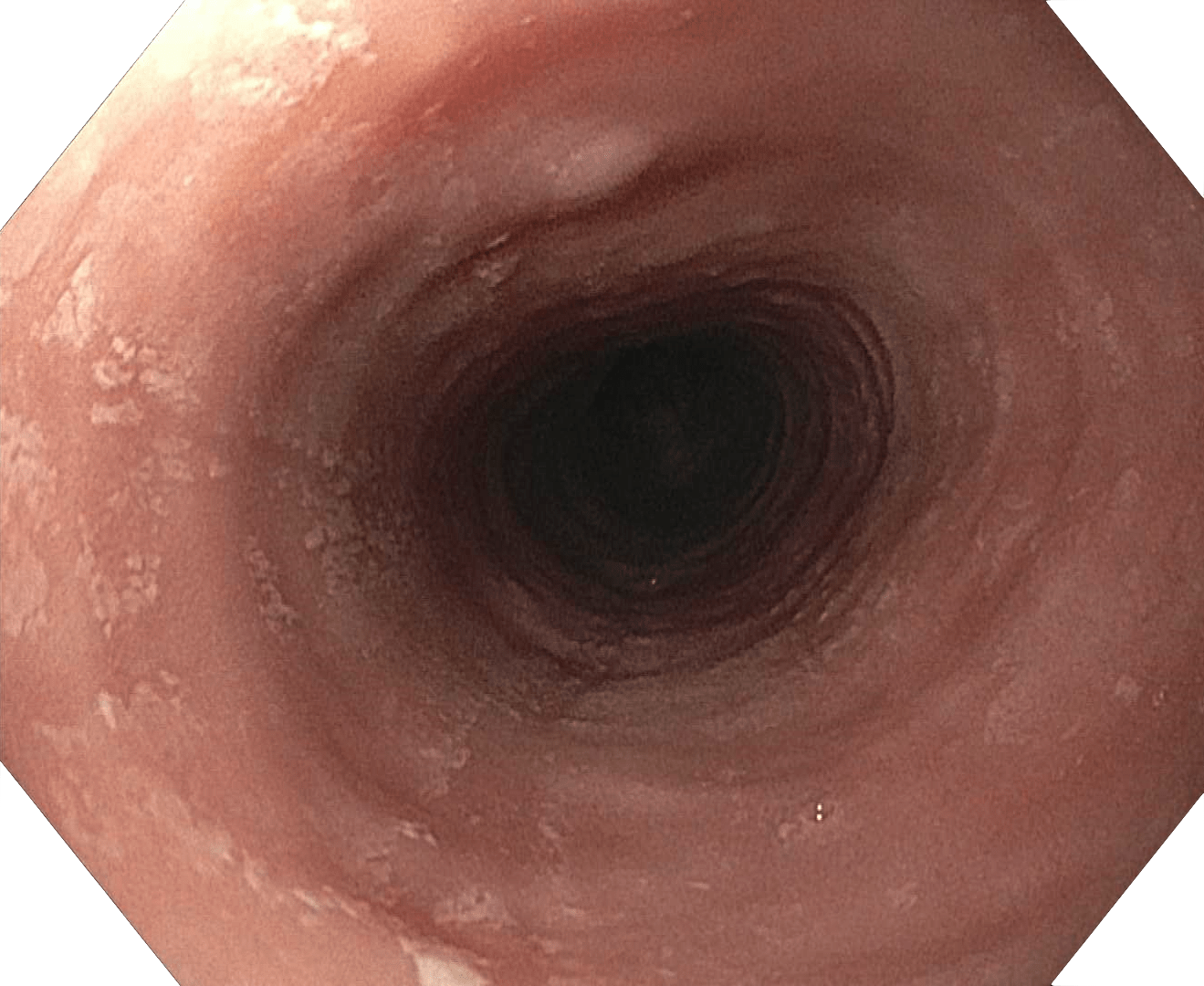
oesophagus with white spots
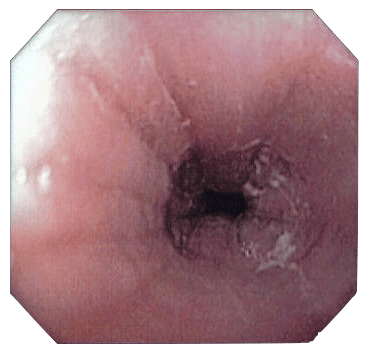
oesophagus with furrowing
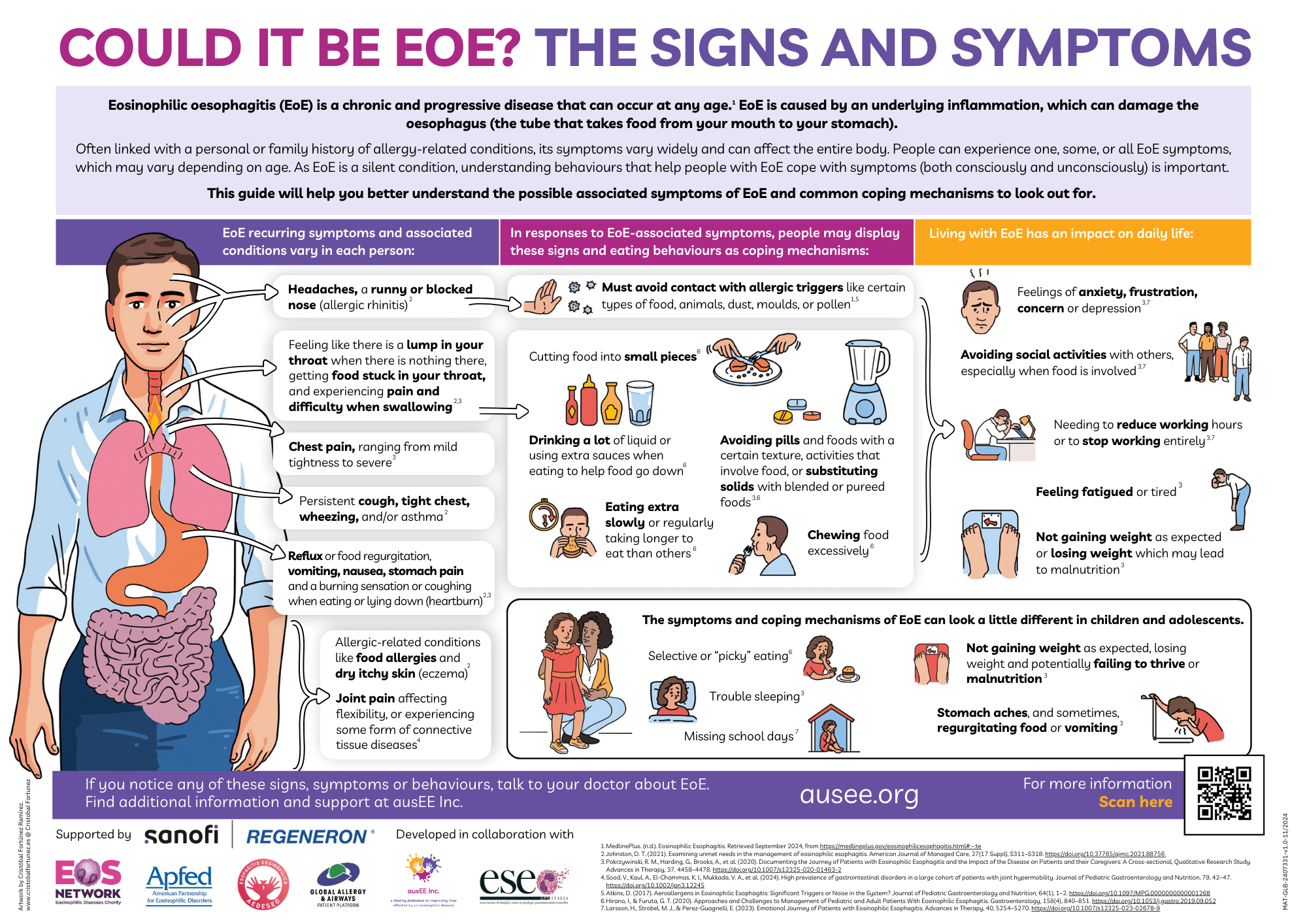
What are the symptoms of EGID & EoE?
The symptoms of EoE vary from one individual to the next and can include:
- Feeding difficulty (such as needing to puree foods, being slow to chew foods, avoidance of textured foods, oral aversion)
- Difficulty in swallowing foods and/or regularly requiring a drink after eating
- A food suddenly becoming stuck in the oesophagus (called a food impaction/food bolus obstruction)
- Nausea, persistent vomiting and retching
- Abdominal (stomach) or chest pain
- Reflux that does not respond to anti-acid medication
- Failure to thrive (failure to put on or loss of weight)
In other types of eosinophilic gastrointestinal diseases, symptoms depend on which part of the gut is affected (e.g. diarrhoea and bloody stools if the small or large intestine is involved).
How is an EGID & EoE Diagnosed?
An endoscopy with biopsies is the only way to confirm the diagnosis of an EGID and EoE at present. The diagnosis cannot be based upon symptoms alone.
Endoscopy – A gastroenterologist performs an endoscopy by using an endoscope (a tube with a light and camera at the end) to look at the GI tract and take small biopsies, usually from the upper oesophagus, lower oesophagus, stomach and duodenum. The oesophagus may look visually normal, but when the tissue is examined under a microscope, an accumulation of eosinophils can be detected. It is also possible that the endoscopist could visually detect rings or furrowing, thickened folds and white plaques.

eosinophils under a microscope
Biopsy – The biopsies taken are later reviewed by a pathologist under a microscope. A high number of eosinophils (counted per high-power field) suggest the diagnosis of an EGID. Eosinophils can normally be found in small numbers in all areas of the GI tract except the oesophagus. GERD/GORD (acid reflux disease) is associated with low numbers of eosinophils in the oesophagus. With EoE, the number of eosinophils seen is much higher and remains elevated despite treatment with acid reflux medication. A minimum of 15 eosinophils per high-power field are required to make the diagnosis of EoE.
The diagnosis of an EGID is often delayed and other reasons for eosinophilic infiltration should be ruled out.
The diagnosis of an EGID is often delayed and other reasons for eosinophilic infiltration should be ruled out.
What is the Treatment for an EGID & EoE?
There is no cure for an EGID and EoE, but the goal of treatment is to eliminate the eosinophils in the affected area, thereby alleviating symptoms and reducing inflammation to minimal safe levels. Treating specialists should discuss the options with patients/families and tailor treatment to the individual. EGIDs are chronic diseases that require ongoing management and monitoring with endoscopies and repeat biopsies. As symptoms can fluctuate, they alone are not a reliable indication of disease control. EoE not treated adequately often leads to worsening of the condition with symptoms such as food impactions becoming more frequent. New monitoring methods and treatment options (including biologic therapies) are on the horizon.
Current treatment options for EoE include: Elimination diet - It is important to speak with an Allergist and/or Gastroenterologist, and have a Dietitian experienced in food allergy before undertaking an elimination diet. Some individuals may be able to identify specific food(s) that trigger symptoms, but most cannot. More than one food may be involved. Some doctors suggest removal of up to six common food allergens (milk, wheat, egg, soy, peanut/tree nut, shellfish/fish). A common approach is the ‘step-up’ elimination diet with at first, only one or two food groups (usually milk/dairy and wheat as the most common triggers) being eliminated and then more if required. Foods outside of the common allergens can also be EoE triggers. There is currently no test (skin prick test, blood test etc.) that can reliably indicate the specific food trigger(s) in EoE. With any elimination diet it is important to ensure diet is balanced, growth is maintained and a plan is in place to re-assess.
Elemental diet – This consists of a special medical food called an elemental/amino acid-based formula. It provides all the nutrition a person needs if enough is taken. Some individuals need a feeding tube to ensure they are getting enough of the formula or to give the oesophagus a rest. The person is placed on the formula alone for a number of weeks and will have a repeat endoscopy. If the condition has improved, then foods are slowly introduced back into the diet and a repeat endoscopy is often performed to ensure ongoing control with food reintroduction.
Medication - The most common medications used in EoE are swallowed corticosteroids, often a fluticasone puffer (which is swallowed), budesonide ampoules (made into a slurry) or budesonide orally disintegrating tablets (for adults). These coat the oesophagus and assist in getting rid of eosinophils. Acid reflux medications/proton pump inhibitors (PPIs) may also be used, as they can decrease eosinophils in addition to their anti-acid effect. The doctor will determine which, if any, medications are appropriate for each individual. Medications can be used alone and/or along with dietary management.
Oesophageal dilation – This can be used in people with severe narrowing or strictures of the oesophagus to provide instant relief, and in those with long-standing symptoms who have tried diet or medications and have not improved. Whilst dilation in EoE is safe, this treatment involves an endoscopic procedure and is best used in carefully selected cases.
Current treatment options for EoE include: Elimination diet - It is important to speak with an Allergist and/or Gastroenterologist, and have a Dietitian experienced in food allergy before undertaking an elimination diet. Some individuals may be able to identify specific food(s) that trigger symptoms, but most cannot. More than one food may be involved. Some doctors suggest removal of up to six common food allergens (milk, wheat, egg, soy, peanut/tree nut, shellfish/fish). A common approach is the ‘step-up’ elimination diet with at first, only one or two food groups (usually milk/dairy and wheat as the most common triggers) being eliminated and then more if required. Foods outside of the common allergens can also be EoE triggers. There is currently no test (skin prick test, blood test etc.) that can reliably indicate the specific food trigger(s) in EoE. With any elimination diet it is important to ensure diet is balanced, growth is maintained and a plan is in place to re-assess.
Elemental diet – This consists of a special medical food called an elemental/amino acid-based formula. It provides all the nutrition a person needs if enough is taken. Some individuals need a feeding tube to ensure they are getting enough of the formula or to give the oesophagus a rest. The person is placed on the formula alone for a number of weeks and will have a repeat endoscopy. If the condition has improved, then foods are slowly introduced back into the diet and a repeat endoscopy is often performed to ensure ongoing control with food reintroduction.
Medication - The most common medications used in EoE are swallowed corticosteroids, often a fluticasone puffer (which is swallowed), budesonide ampoules (made into a slurry) or budesonide orally disintegrating tablets (for adults). These coat the oesophagus and assist in getting rid of eosinophils. Acid reflux medications/proton pump inhibitors (PPIs) may also be used, as they can decrease eosinophils in addition to their anti-acid effect. The doctor will determine which, if any, medications are appropriate for each individual. Medications can be used alone and/or along with dietary management.
Oesophageal dilation – This can be used in people with severe narrowing or strictures of the oesophagus to provide instant relief, and in those with long-standing symptoms who have tried diet or medications and have not improved. Whilst dilation in EoE is safe, this treatment involves an endoscopic procedure and is best used in carefully selected cases.
For more information:
Talk to your doctor about Eosinophilic Gastrointestinal Diseases
References
Australasian Society of Clinical Immunology and Allergy (ASCIA)Consortium of Eosinophilic Gastrointestinal Disease Researchers (CEGIR)Updated International Consensus Diagnostic Criteria for Eosinophilic Esophagitis: Proceedings of the AGREE ConferenceInternational Consensus Recommendations for Eosinophilic Gastrointestinal Disease Nomenclature
ausEE Publications on EGIDs
To receive free printed copies of our patient resources by post please complete our resources order form.
Could it be EoE?
The Signs and Symptoms
EGID Fact Sheet

EGID Information Flyer/Poster

ASCIA Resources for EoE
The following eosinophilic oesophagitis (EoE) resources are available on the Australasian Society of Clinical Immunology and Allergy (ASCIA) website:
- ASCIA Action Plan* for EoE - for emergency treatment of food impaction/food bolus obstruction (FBO) due to EoE
- ASCIA Management Plan* for EoE - to guide ongoing treatment and management of EoE
- ASCIA EoE Frequently Asked Questions (FAQ)
- ASCIA Two Food Elimination Diet (2FED) Dietary Guide for EoE
- ASCIA Four Food Elimination Diet (4FED) Dietary Guide for EoE
These resources were developed by ASCIA involving an extensive review process working with the ASCIA EoE Working Party, ASCIA Paediatric committee and ASCIA Dietitian committee members and ausEE was delighted to be involved throughout the collaboration process.
* Please note that ASCIA Action and Management Plans for EoE are medical documents that can only be completed and signed by the patient's clinical immunology/allergy specialist or gastroenterologist and cannot be altered without their permission. We encourage patients to talk to their treating specialist about these plans and to discuss the dietary guides with their dietitian if they are currently following or plan on following an elimination diet for EoE.
* Please note that ASCIA Action and Management Plans for EoE are medical documents that can only be completed and signed by the patient's clinical immunology/allergy specialist or gastroenterologist and cannot be altered without their permission. We encourage patients to talk to their treating specialist about these plans and to discuss the dietary guides with their dietitian if they are currently following or plan on following an elimination diet for EoE.

Useful Links
American Partnership for Eosinophilic Disorders (APFED) - EGIDS
EOS Aware - My EAD Stories
EOS Network - EoE - Eosinophilic OesophagitisEOS Network - EoG - EoN - EoC Eosinophilic Diseases Lower Gut
Joint ESPGHAN/NASPGHAN Guidelines on Childhood Eosinophilic Gastrointestinal Disorders Beyond Eosinophilic Esophagitis
Rare Awareness Rare Education (RARE) Portal - Eosinophilic gastrointestinal diseases (EGIDs)Rare Awareness Rare Education (RARE) Portal - Eosinophilic oesophagitis (EoE)
Page last modified: 17 December 2025